ETIOLOGY
Unknown
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Although elevated ESR is typical, it may also be normal. Typical changes of the sacroliacal joints in radiographs show narrowing of the joint space along with sclerosing and erosive features (Fig. 4.6), finally leading to ankylosis. Involvement of the spine is characterized by ossification of the ligaments (Fig. 4.7).
• Other spondyloarthropathies
WORKUP
The modified New York criteria are often used for diagnosis:
• Low back pain of at least 3 mo duration improved by exercise and not relieved by rest
• Limitation of lumbar spine movement in sagittal and frontal planes
• Decreased chest expansion below normal values for age and sex
• Bilateral sacroiliitis of minimal grade or greater
• Unilateral sacroiliitis of moderate grade or greater
LABORATORY TESTS
• Elevated sedimentation rate
• Absence of rheumatoid factor and ANA
• Possible mild hyperchromic anemia
• Presence of HLA/B27 antigen in >90% of patients
IMAGING STUDIES
• Early roentgenographic features are those of bilateral sacroiliitis on plain films.
• Vertebral bodies may become de-mineralized and a typical “squaring off” occurs.
• With progression, calcification of the annulus fibrosus and paravertebral ligaments develop, giving rise to the so-called bamboo spine appearance.
• End result may be a forward protruding cervical spine and fixed dorsal kyphosis.
TREATMENT
Because no treatment reliably stops disease progression, management is used to delay further deformity by stressing the importance of good posture, stretching and deep-breathing exercises and, if appropriate, braces and lightweight supports. Heat, warm showers, baths, ice, and nerve stimulation measures may relieve symptoms in some patients. Nonsteroidal anti-inflammatory drugs, such as aspirin, indomethacin, and sulindac, control pain and inflammation. Phenylbutazone may be used in severe cases.
Severe hip involvement, which affects about 15% of patients, usually necessitates hip replacement surgery. Severe spinal involvement may require a spinal wedge osteotomy to separate and reposition the vertebrae. This surgery is reserved for selected patients because of possible spinal cord damage and a lengthy convalescence.
NONPHARMACOLOGIC THERAPY
• Exercises primarily to maintain flexibility; general aerobic activity also important
• Postural training
1. Patients must be instructed to sit in the erect position and to avoid stooping; otherwise, a flexion contracture of the spine may develop, which can become so severe that the patient cannot see forward.
2. Sleeping should be in the supine position on a firm mattress; pillows should not be placed under the head or knees.
CHRONIC Rx
NSAIDs: indomethacin is often successful in relieving symptoms; newer nonsteroidal agents may be tried as well.
• New research into the use of DMARDs such as tumor necrosis factor antagonists such as etanercept appears promising.
DISPOSITION
• Most patients have a normal life span.
• The usual course of the disease is not life-threatening, but death may occur as a result of aortic insufficiency or secondary amyloidosis with renal disease.
REFERRAL
• Orthopedic consultation for pain or deformity
• Ophthalmologic consultation for ocular complications
• Rheumatology consultation for uncontrolled symptoms
Unknown
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Although elevated ESR is typical, it may also be normal. Typical changes of the sacroliacal joints in radiographs show narrowing of the joint space along with sclerosing and erosive features (Fig. 4.6), finally leading to ankylosis. Involvement of the spine is characterized by ossification of the ligaments (Fig. 4.7).
• Other spondyloarthropathies
WORKUP
The modified New York criteria are often used for diagnosis:
• Low back pain of at least 3 mo duration improved by exercise and not relieved by rest
• Limitation of lumbar spine movement in sagittal and frontal planes
• Decreased chest expansion below normal values for age and sex
• Bilateral sacroiliitis of minimal grade or greater
• Unilateral sacroiliitis of moderate grade or greater
LABORATORY TESTS
• Elevated sedimentation rate
• Absence of rheumatoid factor and ANA
• Possible mild hyperchromic anemia
• Presence of HLA/B27 antigen in >90% of patients
IMAGING STUDIES
• Early roentgenographic features are those of bilateral sacroiliitis on plain films.
• Vertebral bodies may become de-mineralized and a typical “squaring off” occurs.
• With progression, calcification of the annulus fibrosus and paravertebral ligaments develop, giving rise to the so-called bamboo spine appearance.
• End result may be a forward protruding cervical spine and fixed dorsal kyphosis.
TREATMENT
Because no treatment reliably stops disease progression, management is used to delay further deformity by stressing the importance of good posture, stretching and deep-breathing exercises and, if appropriate, braces and lightweight supports. Heat, warm showers, baths, ice, and nerve stimulation measures may relieve symptoms in some patients. Nonsteroidal anti-inflammatory drugs, such as aspirin, indomethacin, and sulindac, control pain and inflammation. Phenylbutazone may be used in severe cases.
Severe hip involvement, which affects about 15% of patients, usually necessitates hip replacement surgery. Severe spinal involvement may require a spinal wedge osteotomy to separate and reposition the vertebrae. This surgery is reserved for selected patients because of possible spinal cord damage and a lengthy convalescence.
NONPHARMACOLOGIC THERAPY
• Exercises primarily to maintain flexibility; general aerobic activity also important
• Postural training
1. Patients must be instructed to sit in the erect position and to avoid stooping; otherwise, a flexion contracture of the spine may develop, which can become so severe that the patient cannot see forward.
2. Sleeping should be in the supine position on a firm mattress; pillows should not be placed under the head or knees.
CHRONIC Rx
NSAIDs: indomethacin is often successful in relieving symptoms; newer nonsteroidal agents may be tried as well.
• New research into the use of DMARDs such as tumor necrosis factor antagonists such as etanercept appears promising.
DISPOSITION
• Most patients have a normal life span.
• The usual course of the disease is not life-threatening, but death may occur as a result of aortic insufficiency or secondary amyloidosis with renal disease.
REFERRAL
• Orthopedic consultation for pain or deformity
• Ophthalmologic consultation for ocular complications
• Rheumatology consultation for uncontrolled symptoms
Ankylosing spondylitis (Bekhterev Disease)
BASIC INFORMATION
DEFINITION
Ankylosing spondylitis represents the classical spondylarthropathy. This chronic inflammatory disorder affects sacroiliacal, costovertebral, and facet joints leading to progressive ankylosis. Hips and shoulders are most commonly affected whereas other joints are less often involved. Systemic manifestations are rare (uveitis anterior, aortitis with aortic insufficiency, pulmonary fibrosis). Men are affected more often and more severely than women. First symptoms usually develop between the ages of 20-40. Typical symptoms include low back and buttock pain at night, radiating towards the dorsal aspects of the knees. Motion is followed by decreased pain. Stressing the sacroiliacal joints is painful due to inflammation (Mennel or Patrick sign). Axial involvement often leads to early ankylosis with typical deformities: hyperkyphosis of the thoracic spine, flattening of the lower spine (Fig. 4.5). Plantar and achilles enthesiopathies are frequent origins of heel pain. Hip involvement leads to a tendency towards contracture.
SYNONYMS
Marie-Strumpell disease
Bekhterev Disease
EPIDEMIOLOGY & DEMOGRAPHICS
PREVALENCE: 0.15% of male population (rare in blacks)
PREDOMINANT AGE AT ONSET: 15 to 35 yr
PREDOMINANT SEX: Male:female ratio of 10:1
PHYSICAL FINDINGS & CLINICAL PRESENTATION
• Morning stiffness
• Fatigue, weight loss, anorexia, and other systemic complaints in more severe forms
• Bilateral sacroiliac tenderness (sacroiliitis)
• Limited lumbar spine motion
• Loss of chest expansion measured at the nipple line < 2.5 cm, reflecting rib cage involvement
• Occasionally, peripheral joint involvement (large joints are more commonly affected)
• Possible extraskeletal manifestations affecting the cardiovascular system (aortic insufficiency, heart block, cardiomegaly), lungs (pulmonary fibrosis), and eye (uveitis)
• Tenderness at tendon insertion sites
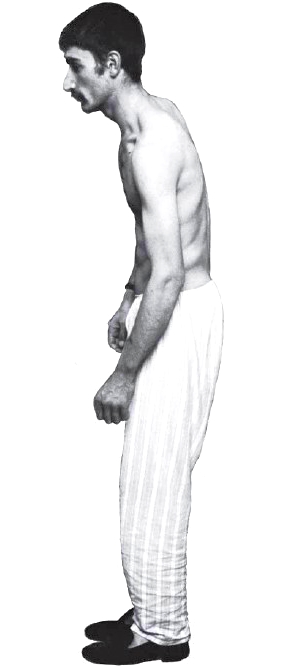
Fig. 4.5 Typical positioning of a patient with Bekhterev disease.
Assessment findings
Varying assessment findings depend on the disease stage. The patient may first complain of intermittent low back pain that is most severe in the morning or after inactivity and is relieved by exercise. He may also report mild fatigue, fever, anorexia, and weight loss. If he has symmetrical or asymmetrical peripheral arthritis, he may describe pain in his shoulders, hips, knees, and ankles.
The patient may also complain of pain over the symphysis pubis, which may lead to its mistaken identity as pelvic inflammatory disease.
Observe the patient's movements. Note stiffness or limited motion of the lumbar spine; pain and limited expansion of the chest, resulting from costovertebral and sternomanubrial joint involvement; and limited range of motion, resulting from hip deformity.
Varying assessment findings depend on the disease stage. The patient may first complain of intermittent low back pain that is most severe in the morning or after inactivity and is relieved by exercise. He may also report mild fatigue, fever, anorexia, and weight loss. If he has symmetrical or asymmetrical peripheral arthritis, he may describe pain in his shoulders, hips, knees, and ankles.
The patient may also complain of pain over the symphysis pubis, which may lead to its mistaken identity as pelvic inflammatory disease.
Observe the patient's movements. Note stiffness or limited motion of the lumbar spine; pain and limited expansion of the chest, resulting from costovertebral and sternomanubrial joint involvement; and limited range of motion, resulting from hip deformity.
Inspect the spine. In advanced disease, expect to see kyphosis (caused by chronic stooping to relieve discomfort). Inspect the eyes for redness and inflammation resulting from iritis.
Palpate affected joints. Note any warmth, swelling, or tenderness. Auscultate the heart and listen for an aortic murmur caused by regurgitation and cardiomegaly. Also auscultate the lungs. When present, upper lobe pulmonary fibrosis, which mimics tuberculosis, may reduce vital capacity to 70% or less of predicted volume.
Palpate affected joints. Note any warmth, swelling, or tenderness. Auscultate the heart and listen for an aortic murmur caused by regurgitation and cardiomegaly. Also auscultate the lungs. When present, upper lobe pulmonary fibrosis, which mimics tuberculosis, may reduce vital capacity to 70% or less of predicted volume.


Fig. 4.6 Sacroiliac joints in Bekhterev disease.
Fig. 4.7 Ossified ligaments along the spine in Bekhterev disease.
Contacts: lubopitno_bg@abv.bg www.encyclopedia.lubopitko-bg.com Corporation. All rights reserved.
DON'T FORGET - KNOWLEDGE IS EVERYTHING!