Table 18.1 Nomenclature of bone tumors
Chickenpox
BASIC INFORMATION
DEFINITION
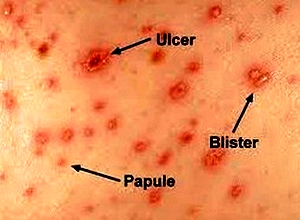
Chickenpox (varicella-zoster virus) is a highly contagious childhood disease. After an incubation period of two to three weeks, a prodromal phase (transient exanthema, limb pain) can occasionally occur. The skin lesions of the varicella exanthema are initially pale pink and transform themselves within a few hours into papules, and later into vesicles which dry after one to two days. The exanthema occurs in several consecutive episodes which are accompanied in each case by a rise in temperature. Therefore, various developmental stages of the skin lesions exist simultaneously. A cervical lymphadenopathy is frequently observed. Complications (bacterial secondary infections, or bullous or necrotizing courses of the disease) are rare.
SYNONYMS
Varicella
EPIDEMIOLOGY & DEMOGRAPHICS
• Chickenpox is extremely contagious. Over 90% of unvaccinated contacts become infected.
• The incubation period of chickenpox ranges from 9 to 21 days.
• Peak incidence is in the springtime.
• The predominant age is 5 to 10 years.
• Infectious period begins 2 days before onset of clinical symptoms and lasts until all lesions have crusted.
• Most patients will have lifelong immunity following an attack of chickenpox; protection from chickenpox following varicella vaccine is approximately 6 years.

PHYSICAL FINDINGS & CLINICAL PRESENTATION
• Findings vary with the clinical course. Initial symptoms consist of fever, chills, backache, generalized malaise, and headache.
• Symptoms are generally more severe in adults.
• Initial lesions generally occur on the trunk (centripetal distribution) and occasionally on the face; these lesions consist primarily of 3- to 4-mm red papules with an irregular outline and a clear vesicle on the surface (dew drops on a rose petal appearance).
• Intense pruritus generally accompanies this stage.
• New lesion development generally ceases by the fourth day with subsequent crusting by the sixth day.
• Lesions generally spread to the face and the extremities (centrifugal spread).
• Patients generally present with lesions at different stages at the same time.
• Crusts generally fall off within 5 to 14 days.
• Fever is usually highest during the eruption of the vesicles; temperature generally returns to normal following disappearance of vesicles.
• Signs of potential complications (e.g., bacterial skin infections, neurologic complications, pneumonia, hepatitis) may be present on physical examination.
• Mild constitutional symptoms (e.g., anorexia, myalgias, headaches, restlessness) may be present (most common in adults).
• Excoriations may be present if scratching is prominent.
ETIOLOGY
Varicella-zoster virus (VZV) is a human herpesvirus III that can manifest with either varicella or herpes zoster (i.e., shingles, which is a reactivation of varicella).
Clinical features of chickenpox
Fourteen to twenty-one days after exposure to VZV, a brief prodromal illness of fever, headache and malaise heralds the eruption of chickenpox, characterized by the rapid progression of macules to papules to vesicles to pustules in a matter of hours (Fig. 66). In young children the prodromal illness may be very mild or absent. The illness tends to be more severe in older children and can be debilitating in adults. The lesions occur on the face, scalp and trunk, and to a lesser extent on the extremities. It is characteristic to see skin lesions at all stages of development on the same area of skin. Fever subsides as soon as new lesions cease to appear. Eventually the pustules crust and heal without scarring. Complications of chickenpox include pneumonia, which generally begins 1-6 days after the skin eruption, and bacterial superinfection of skin lesions. Pneumonia is more common in adults than in children and cigarette smokers are at particular risk. Pulmonary symptoms are usually more striking than the physical findings, although a chest radiograph usually shows diffuse changes throughout both lung fields. CNS involvement occurs in about 1 per 1000 cases and most commonly presents as an acute truncal cerebellar ataxia. The immunocompromised are susceptible to disseminated infection with multiorgan involvement. Women in pregnancy are prone to severe chickenpox and, in addition, there is a risk of intrauterine infection with structural damage to the fetus (if maternal infection is within the first 20 weeks of pregnancy, the risk of varicella embryopathy is 1-2%).
• Findings vary with the clinical course. Initial symptoms consist of fever, chills, backache, generalized malaise, and headache.
• Symptoms are generally more severe in adults.
• Initial lesions generally occur on the trunk (centripetal distribution) and occasionally on the face; these lesions consist primarily of 3- to 4-mm red papules with an irregular outline and a clear vesicle on the surface (dew drops on a rose petal appearance).
• Intense pruritus generally accompanies this stage.
• New lesion development generally ceases by the fourth day with subsequent crusting by the sixth day.
• Lesions generally spread to the face and the extremities (centrifugal spread).
• Patients generally present with lesions at different stages at the same time.
• Crusts generally fall off within 5 to 14 days.
• Fever is usually highest during the eruption of the vesicles; temperature generally returns to normal following disappearance of vesicles.
• Signs of potential complications (e.g., bacterial skin infections, neurologic complications, pneumonia, hepatitis) may be present on physical examination.
• Mild constitutional symptoms (e.g., anorexia, myalgias, headaches, restlessness) may be present (most common in adults).
• Excoriations may be present if scratching is prominent.
ETIOLOGY
Varicella-zoster virus (VZV) is a human herpesvirus III that can manifest with either varicella or herpes zoster (i.e., shingles, which is a reactivation of varicella).
Clinical features of chickenpox
Fourteen to twenty-one days after exposure to VZV, a brief prodromal illness of fever, headache and malaise heralds the eruption of chickenpox, characterized by the rapid progression of macules to papules to vesicles to pustules in a matter of hours (Fig. 66). In young children the prodromal illness may be very mild or absent. The illness tends to be more severe in older children and can be debilitating in adults. The lesions occur on the face, scalp and trunk, and to a lesser extent on the extremities. It is characteristic to see skin lesions at all stages of development on the same area of skin. Fever subsides as soon as new lesions cease to appear. Eventually the pustules crust and heal without scarring. Complications of chickenpox include pneumonia, which generally begins 1-6 days after the skin eruption, and bacterial superinfection of skin lesions. Pneumonia is more common in adults than in children and cigarette smokers are at particular risk. Pulmonary symptoms are usually more striking than the physical findings, although a chest radiograph usually shows diffuse changes throughout both lung fields. CNS involvement occurs in about 1 per 1000 cases and most commonly presents as an acute truncal cerebellar ataxia. The immunocompromised are susceptible to disseminated infection with multiorgan involvement. Women in pregnancy are prone to severe chickenpox and, in addition, there is a risk of intrauterine infection with structural damage to the fetus (if maternal infection is within the first 20 weeks of pregnancy, the risk of varicella embryopathy is 1-2%).

Fig. 66 Chickenpox in an adult. Generalized VZV.
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
• Other viral infection
• Impetigo
• Scabies
• Drug rash
• Urticaria
• Dermatitis herpetiformis
• Smallpox
WORKUP
Diagnosis is usually made based on patient’s history and clinical presentation.
LABORATORY TESTS
• Laboratory evaluation is generally not necessary.
• CBC may reveal leukopenia and thrombocytopenia.
• Serum varicella titers (significant rise in serum varicella IgG antibody level), skin biopsy, or Tzanck smear are used only when diagnosis is in question.
TREATMENT
NONPHARMACOLOGIC THERAPY
• Use antipruritic lotions for symp-tomatic relief.
• Avoid scratching to prevent excoriations and superficial skin infections.
• Use a mild soap for bathing; hands should be washed often.
ACUTE GENERAL Rx
• Use acetaminophen for fever and myalgias; aspirin should be avoided because of the increased risk of Reye’s syndrome.
• Oral acyclovir (20 mg/kg qid for 5 days) initiated at the earliest sign (within 24 hours of illness) is useful in healthy, nonpregnant individuals 13 years of age or older to decrease the duration and severity of signs and symptoms. Immunocompromised hosts should be treated with IV acyclovir 500 mg/m or 10 mg/kg q8h iv for 7 to 10 days.
• Varicella-zoster immunoglobulin (VZIG) is effective in preventing chickenpox in susceptible individuals. Dose is 12.5 U/kg Im (up to a maximum of 625 U). May repeat dose 3 weeks later if the exposure persists; VZIG must be administered as early as possible after presumed exposure.
• Varicella vaccine is available for children and adults; protection lasts at least 6 yr. Patients with HIV or other immunocompromised patients should not receive the live attenuated vaccine.
• Pruritus from chickenpox can be controlled with antihistamines (e.g., hydroxyzine 25 mg q6h) and oral antipruritic lotions (e.g., calamine).
• Oral antibiotics are not routinely indicated and should be used only in patients with secondary infection and infected lesions (most common infective organisms are streptococcus sp. and staphylococcus sp.).
DISPOSITION
• The course is generally benign in immunocompetent adults and children.
• Infants who develop chickenpox are incapable of controlling the infection and should be given varicella-zoster immunoglobulin or globulin if VZIG is not available.
REFERRAL
Hospitalization and IV acyclovir are recommended for immunocompromised patients with chickenpox and for patients who develop neurologic complications or pneumonia.
DIFFERENTIAL DIAGNOSIS
• Other viral infection
• Impetigo
• Scabies
• Drug rash
• Urticaria
• Dermatitis herpetiformis
• Smallpox
WORKUP
Diagnosis is usually made based on patient’s history and clinical presentation.
LABORATORY TESTS
• Laboratory evaluation is generally not necessary.
• CBC may reveal leukopenia and thrombocytopenia.
• Serum varicella titers (significant rise in serum varicella IgG antibody level), skin biopsy, or Tzanck smear are used only when diagnosis is in question.
TREATMENT
NONPHARMACOLOGIC THERAPY
• Use antipruritic lotions for symp-tomatic relief.
• Avoid scratching to prevent excoriations and superficial skin infections.
• Use a mild soap for bathing; hands should be washed often.
ACUTE GENERAL Rx
• Use acetaminophen for fever and myalgias; aspirin should be avoided because of the increased risk of Reye’s syndrome.
• Oral acyclovir (20 mg/kg qid for 5 days) initiated at the earliest sign (within 24 hours of illness) is useful in healthy, nonpregnant individuals 13 years of age or older to decrease the duration and severity of signs and symptoms. Immunocompromised hosts should be treated with IV acyclovir 500 mg/m or 10 mg/kg q8h iv for 7 to 10 days.
• Varicella-zoster immunoglobulin (VZIG) is effective in preventing chickenpox in susceptible individuals. Dose is 12.5 U/kg Im (up to a maximum of 625 U). May repeat dose 3 weeks later if the exposure persists; VZIG must be administered as early as possible after presumed exposure.
• Varicella vaccine is available for children and adults; protection lasts at least 6 yr. Patients with HIV or other immunocompromised patients should not receive the live attenuated vaccine.
• Pruritus from chickenpox can be controlled with antihistamines (e.g., hydroxyzine 25 mg q6h) and oral antipruritic lotions (e.g., calamine).
• Oral antibiotics are not routinely indicated and should be used only in patients with secondary infection and infected lesions (most common infective organisms are streptococcus sp. and staphylococcus sp.).
DISPOSITION
• The course is generally benign in immunocompetent adults and children.
• Infants who develop chickenpox are incapable of controlling the infection and should be given varicella-zoster immunoglobulin or globulin if VZIG is not available.
REFERRAL
Hospitalization and IV acyclovir are recommended for immunocompromised patients with chickenpox and for patients who develop neurologic complications or pneumonia.
Contacts: lubopitno_bg@abv.bg www.encyclopedia.lubopitko-bg.com Corporation. All rights reserved.
DON'T FORGET - KNOWLEDGE IS EVERYTHING!